病因學Etiology
病因學EtiologyMajor depressive disorder (MDD) 主要憂鬱症 is characterized by depressed mood most of the time for at least 2 weeks and/or loss of interest or pleasure in most activities.
There has been a marked shift in the last decade in our understanding of the pathophysiology of major depression.
對憂鬱症而言,神經假說之演變在過去百年間,隨著組織學生理證據而演替
In addition to the older idea that a deficit in function or amount of monoamines (the monoamine hypothesis 單胺假說) is central to the biology of depression, there is evidence that neurotrophic 親神經性的;神經滋養的 and endocrine factors play a major role (the neurotrophic hypothesis 神經滋養假說). 神經滋養假說為上個百年間主流的憂鬱症病因學之主危險因子
Histologic 組織學的studies, structural and functional brain imaging research, genetic findings, and steroid research all suggest a complex pathophysiology for MDD with important implications for drug treatment
There is substantial evidence that nerve growth factors 神經生長因子 such as brain-derived neurotrophic factor (BDNF) are critical in the regulation of neural plasticity可塑性;適應性, resilience 復原力, and neurogenesis 神經生成作用.
在組織學更新證據後,BDNF神經生長因子(位於皮質區/海馬迴等)相關之神經生成作用缺損為憂鬱症病因學新顯學假說
The evidence suggests that depression is associated with the loss of neurotrophic support and that effective antidepressant therapies increase neurogenesis and synaptic connectivity in cortical areas 皮質區 such as the hippocampus 海馬迴.
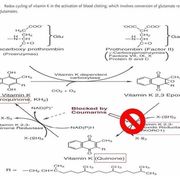
BDNF is thought to exert its influence on neuronal survival and growth effects by activating the tyrosine kinase receptor B in both neurons and glia (Figure 30–1)而抗憂鬱症藥物能顯著影響神經復原/生成,並影響單胺等神經傳遞物質生成與作用而治癒憂鬱症.
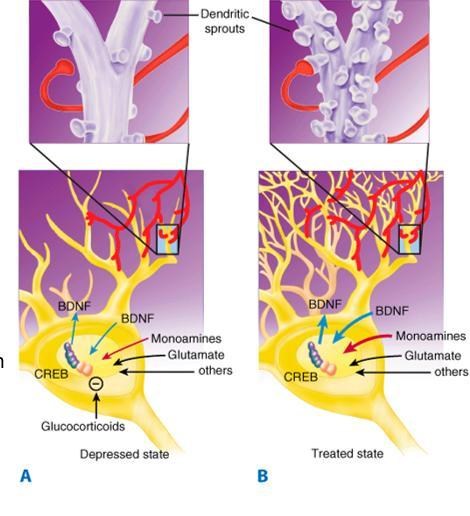
Animal and human studies indicate that stress and pain are associated with a drop in BDNF levels and that this loss of neurotrophic support contributes to atrophic 萎縮的 structural changes in the hippocampus and perhaps other areas such as the medial frontal 前額的 cortex and anterior cingulate 前帶.
超過 30 項大腦內結構成像研究表明,重度憂鬱症與海馬迴體積減少 5-10% 相關,
儘管一些研究與這一發現不相符合。但以醫學統計角度而言,憂鬱和慢性壓力狀態也與anterior cingulate 前帶和 medial frontal 內側眶額皮質的體積大量減少有關。
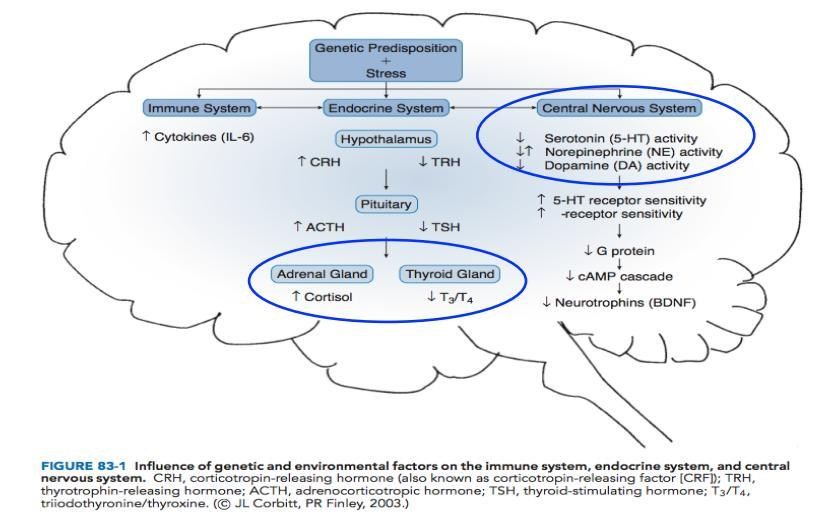
The hippocampus is known to be important both in contextual memory and regulation of the hypothalamic-pituitary-adrenal (HPA) axis & the anterior cingulate plays a role in the integration of emotional stimuli and attention functions, whereas the medial orbital frontal cortex is also thought to play a role in memory, learning, and emotion.
Over 30 structural imaging studies suggest that major depression is associated with a 5–10% loss of volume in the hippocampus, although some studies have not replicated this finding.
Depression and chronic stress states have also been associated with a substantial loss of volume in the anterior cingulate and medial orbital frontal cortex.
Epidemiology流行病學憂鬱症的終生盛行率約 5%-17%,女性有較高的危險性,盛行率是男性的1.7-2.7倍,在65歲-80歲女性約20.4%,男性則為9.6%
• 憂鬱症可以發生在任何年齡,18歲-29歲的成人發生率最高
• 憂鬱症及自殺有家族傾向
• 大約8%-18%的憂鬱症病人其一等親(父母、手足、子女)有憂鬱症病史,而無憂鬱症者則只有5.6%
• 憂鬱症病人的一等親(父母、手足、子女)罹患憂鬱症的危險比一般人高1.5-3倍
• 最近的研究顯示,憂鬱症的致病因素中,基因佔37%、特定的個人因素差異則佔63%且女性較男性常見
診斷標準Disorder Diagnostic Criteria (DSM-5)情緒症狀
1.憂鬱情緒
2.喪失興趣或愉悅感
3.顯著的體重減少或增加
4.失眠或嗜睡
5.精神運動性激動或遲滯
6.疲倦或沒有力氣
7.覺得沒有價值,或過度罪惡感
8.思考或專注能力的下降
9.反覆出現自殺意念、企圖
並且排除物質濫用或其它身體疾病造成的
以上9含有5,且必須包含1或2
幾乎每天大多數時間,症狀會影響到社會、職業、學校、個人功能等因素
藥物治療期間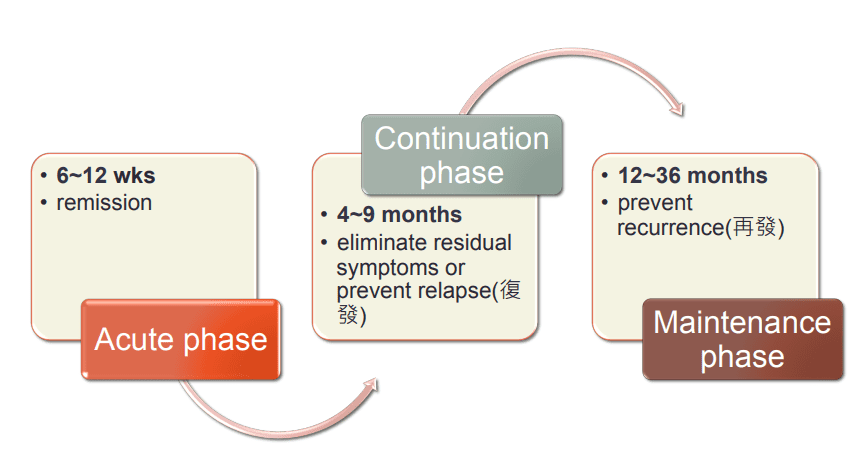
定義:Relapse(復發): return of symptoms within 6 months of remission
Recurrence(再發): a separate episode of depression
General Approach to Treatment
• 抗憂鬱藥治療的時間長短視再發(recurrence)風險而定(過去發作事件數)
• 再發(recurrence)風險最高者,需終身服藥: <40 yrs & ≥ 2 episodes, any age & ≥3 episodes
• 復發(relapse)高風險者,至少服藥2年以上
• 衛教病人和家屬有關抗憂鬱藥需要2-4週以上才會出現效果,及服藥配合度對治療的重要性
藥物化學結構Pharmaceutical Chemistry◆總論
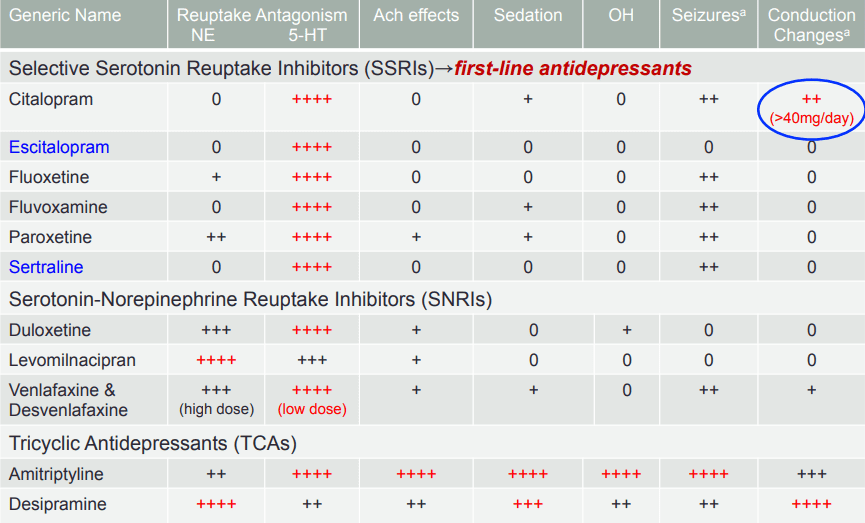
◆Selective serotonin reuptake inhibitors (SSRIs)
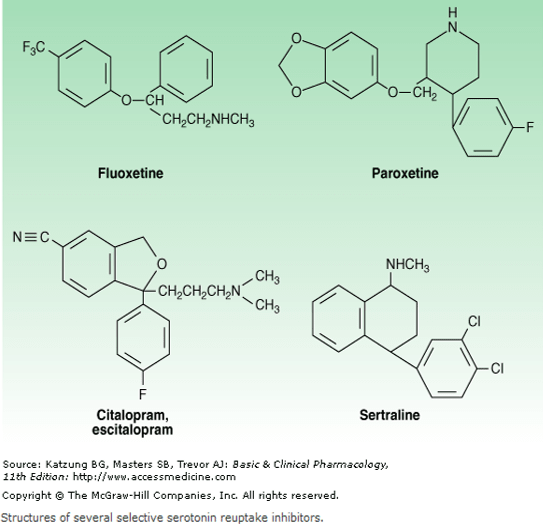
•Fluoxetine, sertraline, and citalopram exist as isomers and are formulated in the racemic 消旋 forms, whereas paroxetine and fluvoxamine are not optically active & escitalopram is the S enantiomer of citalopram.
•As with all antidepressants, SSRIs are highly lipophilic the popularity 流行of SSRIs stems 起源 largely from their ease of use, safety in overdose, relative tolerability 可容忍的, cost (all except escitalopram are generically available), and broad spectrum of uses.
因為是老藥物,整體都較廉價安全.副作用也較可容忍,能增加病患服藥順從性(Drug compliance)
◆SNRIs(serotonin-norepinephrine reuptake inhibitors)
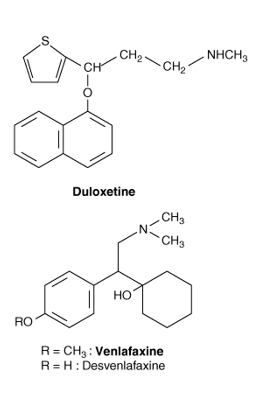
•Two classes of antidepressants act as combined serotonin and norepinephrine reuptake inhibitors: selective serotonin-norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs).
可選擇性抑制血清素-正腎上腺素再回收
•The SNRIs include venlafaxine, its metabolite desvenlafaxine, and duloxetine & milnacipran, is in late clinical trials in the USA but has been available in Europe for several years.
•In addition to their use in major depression, other applications of the SNRIs include the treatment of pain disorders including neuropathies and fibromyalgia; generalized anxiety, stress urinary incontinence, and vasomotor symptoms of menopause.
•SNRIs are chemically unrelated to each other all SNRIs bind the serotonin (SERT) and norepinephrine (NET) transporters, as do the TCAs & however, unlike the TCAs, the SNRIs do not have much affinity for other receptors.SNRI對其他受體無親和力,對血清素與正腎上腺素受體有較高親和力,而抑制兩種再吸收
•Venlafaxine and desvenlafaxine are bicyclic compounds, whereas duloxetine is a three-ring structure unrelated to the TCAs & milnacipran contains a cyclopropane ring and is provided as a racemic mixture.
◆TCAs (tricyclic antidepressants )
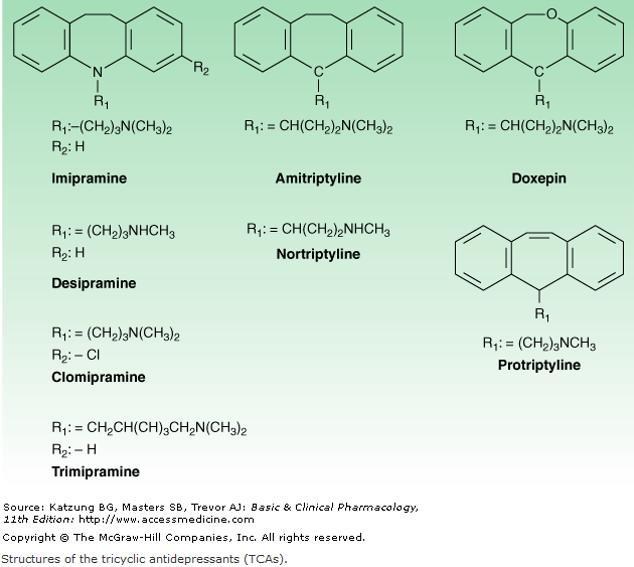
For example, imipramine is highly anticholinergic and is a relatively strong serotonin as well as norepinephrine reuptake inhibitor in contrast, Desipramine is much less anticholinergic and is a more potent and somewhat more selective norepinephrine reuptake inhibitor than is imipramine.
At the present time, the TCAs are used primarily in depression that is unresponsive to more commonly used antidepressants such as the SSRIs or SNRIs & other uses for TCAs include the treatment of pain conditions, enuresis 尿失禁, and insomnia 失眠
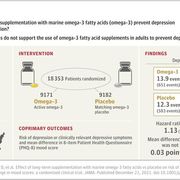
魚油中omega-3的臨床試驗結果德國Duisburg-Essen大學的Christoph Diener博士報告:一些可能影響憂鬱症非藥物治療補充之臨床實踐的最新研究。
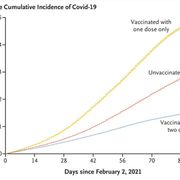
他收集JAMA上一項隨機、安慰劑對照研究,對近 20000 名患者進行魚油中omega3不飽和脂肪酸是否對憂鬱症風險有影響(預防憂鬱症)結果是否定的!
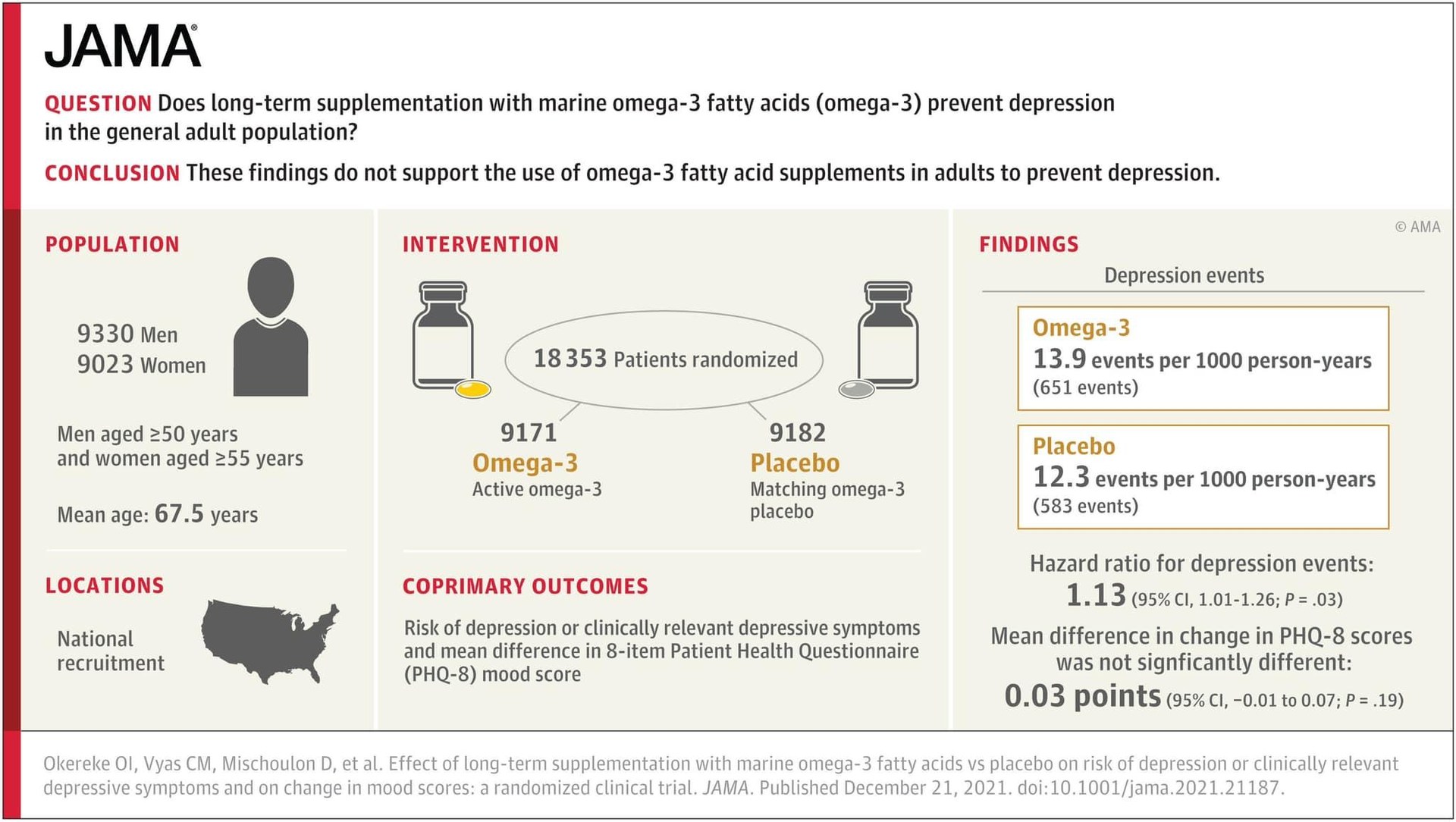
Hazard Ratio反而比安慰劑更高,p value也沒有顯著統計學上價值,故EBM結果為無影響。
不過他隨後也在在 Medline 上進行了文獻檢索,其中列出了 33000 篇關於 omega-3 不飽和酸補充劑和不同疾病的論文:
▪他發現流行病學的研究表明 omega-3 可能有益的疾病:心血管疾病、脂質紊亂、2 型糖尿病、癌症、化療的耐受性、阿茲海默症、憂鬱症、心衰竭、腰椎間盤突出、更年期困擾和經前症候群、類風濕性關節炎、牙周炎、視網膜病變和非酒精性脂肪肝。
這些研究指出,格陵蘭和阿拉斯加的因紐特人社區(Inuit communities)儘管吃肉和大量的魚,但心血管疾病的發病率卻低得驚人。 研究者們解釋是魚中所含的 omega-3 脂肪酸可以降低脂質並提供心臟保護作用。
Diener博士經由omega-3補充劑文獻閱讀,集中在與神經病理學相關的疾病上。
而在審視文獻中,發現在心血管疾病領域,對86項研究進行了統合分析Meta Analysis,約有162000名患者將omega-3與安慰劑進行比較:
▪它對心肌梗死及中風或短暫性腦缺血發作的總體死亡率沒有益處。
▪唯一的趨勢是冠心病患者的死亡率下降,但需要治療的人數(NNT)是334。在EBM醫學實證中是非常不足的樣本數
(NNT: Numbers Needed to Treat)
最後,他檢視並審閱了有關預防和治療憂鬱症和焦慮症的文獻,發現31 項研究涉及超過 50000 人 :
令人震驚的是,同樣omega3對這些疾病沒有任何益處。
Christoph Diener博士認為醫學研究者/第一線醫護人員要吸取的科學教訓是:
即使你在大規模流行病學研究中看到關聯,這並不意味著存在因果關係。
流行病學研究存在嚴重偏見時,文獻也是沒什麼價值的!
例如:Selection Basis選擇偏差
在針對心血管疾病,有能力額外服用 omega-3 脂肪酸的人可能較有可能來自:高收入人群(場外蚵粉)
.並且擁有較健康的生活方式.更經常運動。
因此4%不用擔心,可以繼續在網路上稱王稱霸不用怕買不起房血脂超標憂鬱症!
文獻/圖片來源
1.https://www.medscape.com/viewarticle/9666832.doi:10.1001/jama.2021.21187
3.Basic and Clinical Pharmacology 11th Edition(Copyright: McGraw- Hill Companies)